What Are the Cranial Nerves?
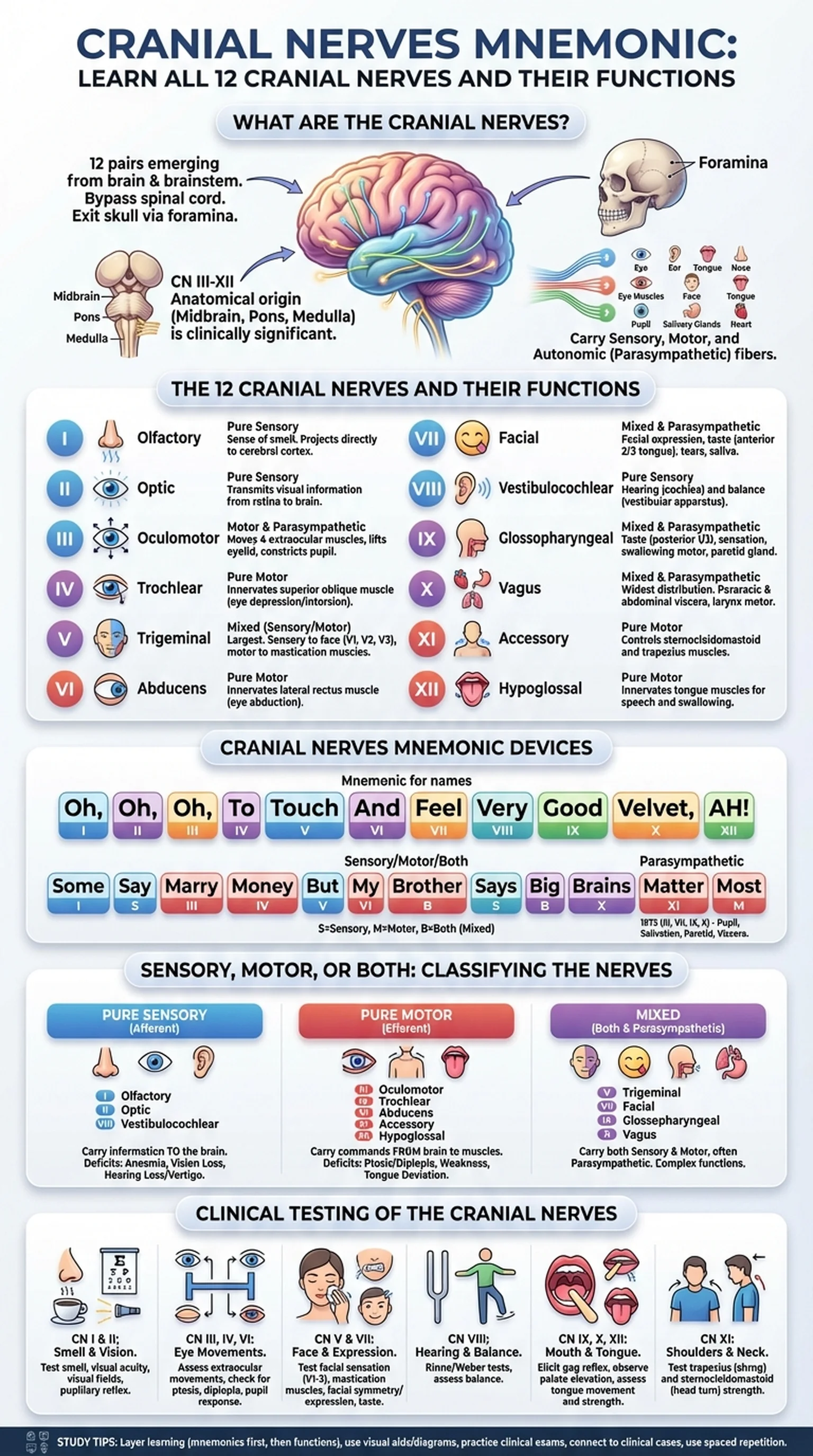
The cranial nerves are twelve pairs of nerves that emerge directly from the brain and brainstem, bypassing the spinal cord to innervate structures primarily in the head and neck. Unlike spinal nerves, which exit through the vertebral column, the cranial nerves pass through foramina (openings) in the skull to reach their target tissues. A thorough understanding of the 12 cranial nerves is essential for students of anatomy, neuroscience, and clinical medicine.
Each cranial nerve is designated by a Roman numeral (I through XII) based on the order in which it exits the brain, from anterior to posterior. Cranial nerve I (olfactory) and cranial nerve II (optic) are unique in that they emerge from the cerebrum and diencephalon, respectively, rather than the brainstem. Cranial nerves III through XII arise from the midbrain, pons, or medulla oblongata. This anatomical origin has clinical significance: a lesion in the midbrain may affect CN III, while a medullary stroke may impair CN IX, X, XI, or XII.
The cranial nerves carry sensory information (such as vision, hearing, taste, and smell), motor commands (to muscles of the eyes, face, tongue, and pharynx), and autonomic (parasympathetic) fibers that regulate pupil constriction, salivation, lacrimation, and visceral organ function. Some cranial nerves are purely sensory (I, II, VIII), some are purely motor (III, IV, VI, XI, XII), and others are mixed, carrying both sensory and motor fibers (V, VII, IX, X). This sensory-motor classification is itself a popular exam topic and the subject of its own cranial nerves mnemonic.
Learning the cranial nerves is a rite of passage in medical and health sciences education. The volume of detail—names, numbers, functions, pathways, foramina, and clinical correlations—can feel overwhelming. That is precisely why cranial nerves mnemonic devices have been used by generations of students to organize and retain this information. With the right mnemonics and a structured study approach, you can master the 12 cranial nerves efficiently and apply your knowledge in clinical settings.
Key Terms
Twelve pairs of nerves that arise directly from the brain and brainstem, innervating structures of the head, neck, and (in the case of CN X) thoracic and abdominal viscera.
An opening or passage in a bone through which a cranial nerve, blood vessel, or other structure passes; plural: foramina.
The posterior part of the brain consisting of the midbrain, pons, and medulla oblongata, from which cranial nerves III–XII originate.
Autonomic nerve fibers carried by certain cranial nerves (III, VII, IX, X) that regulate involuntary functions such as pupil constriction, glandular secretion, and heart rate.